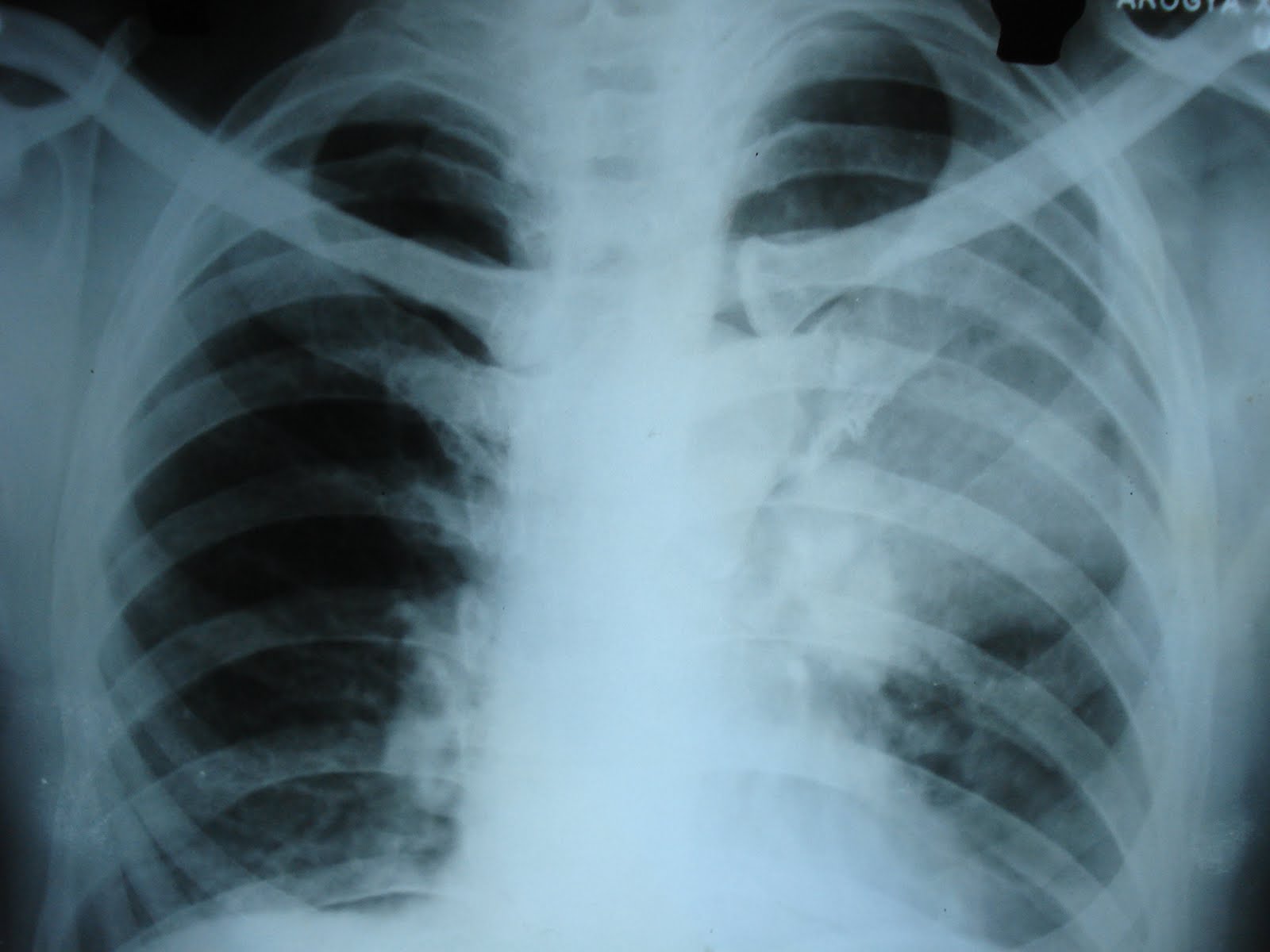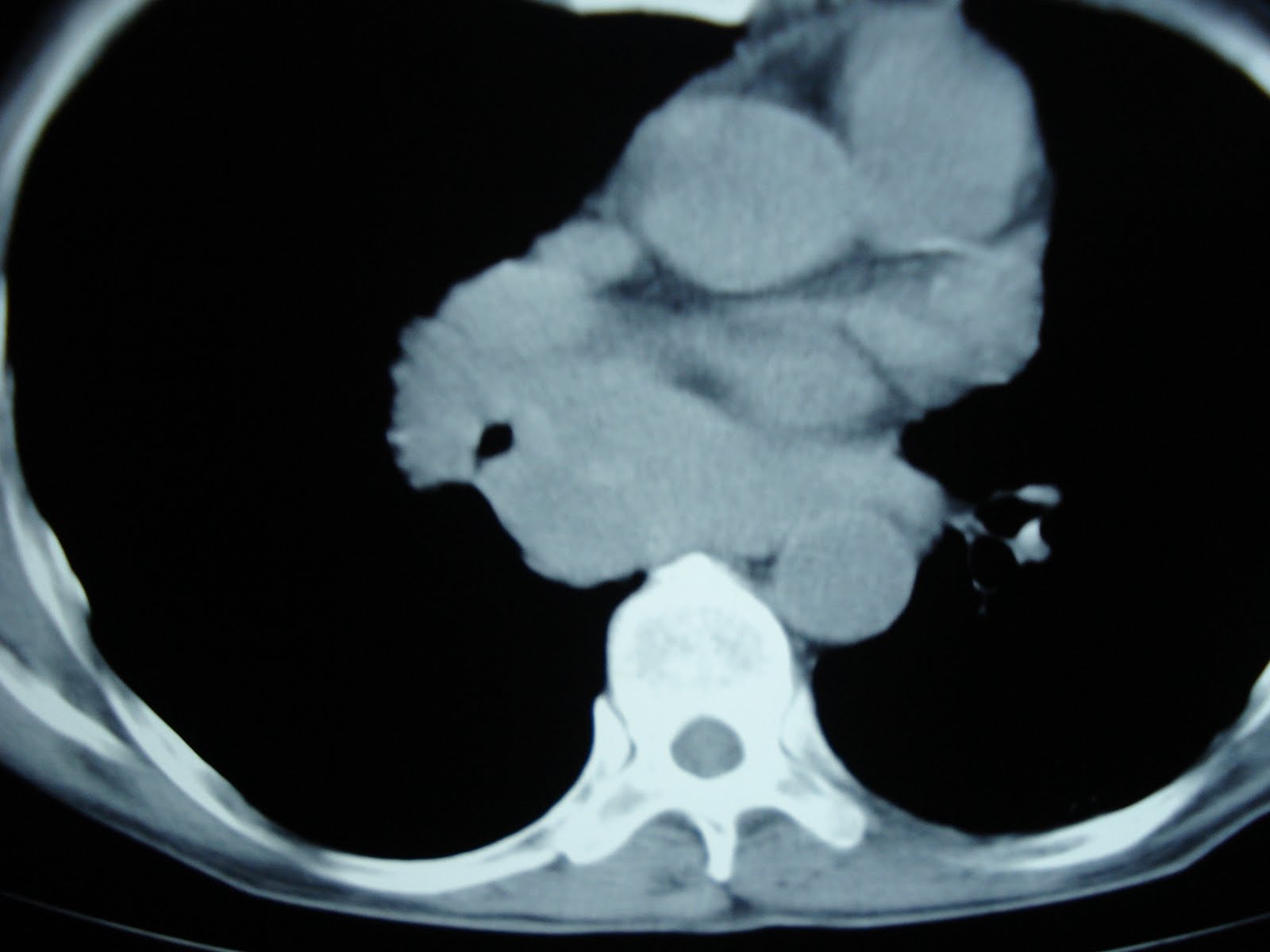

a 50 year old man presented with acute onset shortness of breath since last 5 days which was associated with central chest discomfort for the first 2-3 days. The shortness of breath became agravated intermittently,mainly after prolonged lying down, got relief within a few minutes after sitting up.He had mild cough and was febrile initially.He had no past history of hypertension or diabetes.He had a past history of pulmonary TB which was adequately treated. He was a non smoker and coal miner by occupation. His investigations revealed TLC-14300,n82,L16,E2,ESR65,fbs105,ppbs176,urea41,cr1.6.His troponin T was positive. His chest xray pa view revealed an illdefined rounded mass in left upper lobe and left lateral view revealed a subcarinal rounded mass. CT chest and upper abdomen showed a large calcified mass in left upper lobe of lung and left lobe of liver. There was also a large subcarinal lymph node and bilateral emphysematous changes.We plan to do a bronchoscopy followed by trans bronchial needle aspiration of the subcarinal node to reach a final tissue diagnosis.
http://www.sustain2green.com/